This is an online E-log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.


This E log book also reflects my patient centered online learning portfolio and your valuable comments on comment box is welcome.
I've been given this case to solve in an attempt to understand the topic of "Patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and prognosis
CASE PRESENTATION
A 32yr old Male resident of Miryalguda came to causality with chief complaints of Fever since 7 days
Pain in abdomen since 7 days
Burning micturition since 3 days
𝐇𝐈𝐒𝐓𝐎𝐑𝐘 𝐎𝐅 𝐏𝐑𝐄𝐒𝐄𝐍𝐓𝐈𝐍𝐆 𝐈𝐋𝐋𝐍𝐄𝐒𝐒 :-
Patient was apparently asymptomatic 7 days back then he developed fever which is sudden in onset,high grade , associated with chills and rigors, releived by taking medication and no aggregating factors.pricking type of pain in the abdomen since 7 days in right hypochondriac,right lumbar, umbilical region, aggrevated during deep inspiration.
H/o burning micturition since 3 days,no urgency , frequency, hesitancy.
No chest pain,sob, palpitations
No nausea, vomiting
No loose stools
No increased or decreased output
𝐇𝐈𝐒𝐓𝐎𝐑𝐘 𝐎𝐅 𝐏𝐀𝐒𝐓 𝐈𝐋𝐋𝐍𝐄𝐒𝐒 :
Not k/c/o HTN, DM, TB, EPILEPSY, CVA, CAD.
FAMILY HISTORY: not significant
𝐏𝐄𝐑𝐒𝐎𝐍𝐀𝐋 𝐇𝐈𝐒𝐓𝐎𝐑𝐘 :
Appetite:- normal
Diet:- mixed
Sleep :- adequate
Bowel and bladder movements:- regular
No drug allergies present
He used to take khaini 3-4 times per day since 7 years.
Consumes 180 ml brandy occasionally one time in the evening time every 4 days since 7 years.
No tobacco smoking and chewing.
General examination:
Patient is conscious, coherent, cooperative well oriented to time, place and person .
Moderately built, moderately nourished
Pallor:- absent
Icterus:- absent
Cyanosis:- absent
Clubbing:- absent
Generalized lymphadenopathy:- absent
Bilateral pedal edema :- absent
O/E :
Temp:- 101 F
PR- 72 bpm
BP- 130/90 mm of Hg
Spo2- 98% at room air
RR : 16 cpm
GRBS- 121 mg%
Respiratory system examination :
Inspection :
Position of trachea central
Slight dropping of right shoulder
No intercostal indrawing
No supraclavicular hallowness
Shape and symmetry of the chest normal.
No dilated veins.
No visible scars.
accessory muscles of respiration not prominent.
Palpation :
On three finger test : position of the trachea central.
Respiratory movements are decreased on right side.
Measurement of left and right hemithorax :
47cm equal on bothsides.
Antero posterior diameter :23cm
Transverse diameter at the level of nipples :31.5cm
AP/transverse diameter ratio = 5.75/7.87.
Distance between vertebrae and infrascapular angle on right and left side is same =13.5cm.
Vocal framitus : Right left
Supraclavicular area. Reduced N
Infraclavicular area. Reduced. N
Mammary area. Reduced. N
Axillary area Reduced. N
Infraxillary area Reduced. N
Suprascapular area. Reduced. N
Interscapular area. Reduced. N
Infrascapular area. Reduced. N
Percussion :
On direct percussion in clavicular area
On right side :
On left side :
Tidal percussion: dullness in the right 5 th intercostal space even after deep inspiration.
Traubes space percussion : dull note
Ascultation :
Vocal resonence :
Right left
Supraclavicular area. Reduced N
Infraclavicular area. Reduced N
Mammary area. Reduced N
Axillary area Reduced N
Infraxillary area Reduced N
Suprascapular area. Reduced N
Interscapular area. Reduced N
Infrascapular area. Reduced N
Decreased vesicular breath sounds on right side.
Bilateral air entry positive.
No crackles heard.
On abdominal examination:
Inspection:
Shape of abdomen is scaphoid
Flanks are free
Umblicus is in position, inverted
Skin over abdomen normal shiny, no scars, no sinuses, no nodules, no puncture marks.
No visible veins.
No engorged veins.
Movements of abdominal wall are normal, no visible gastric peristalsis
Palpation:
Liver examination:
On superficial palpation
no tenderness , raised temperature
On deep palpation
No tenderness in liver
Non pulsatile
Spleen examination:
No tenderness and pain
Percussion :
No fluid thrill.
No shifting dullness.
Percussion of Liver for Liver Span : 13cm
Auscultation
Normal bowel sounds heard.
2. Bruit - no renal artery bruit heard.
no iliac artery bruit heard.
CVS Examination :
Inspection :
No abnormal palsations
No visible scars.
No chest deformities.
Mediastinum normal
Trachea central in position.
Palpation :
Mediastinal position : apex beat normal .
Position of trachea central.
Percussion :
On percussion No cardiomegaly.
Ascultation :
on examination of mitral area, pulmonary area, tricuspid area and aortic area S1 and S2 heard. No murmurs heard.
CNS : NAD
INVESTIGATIONS
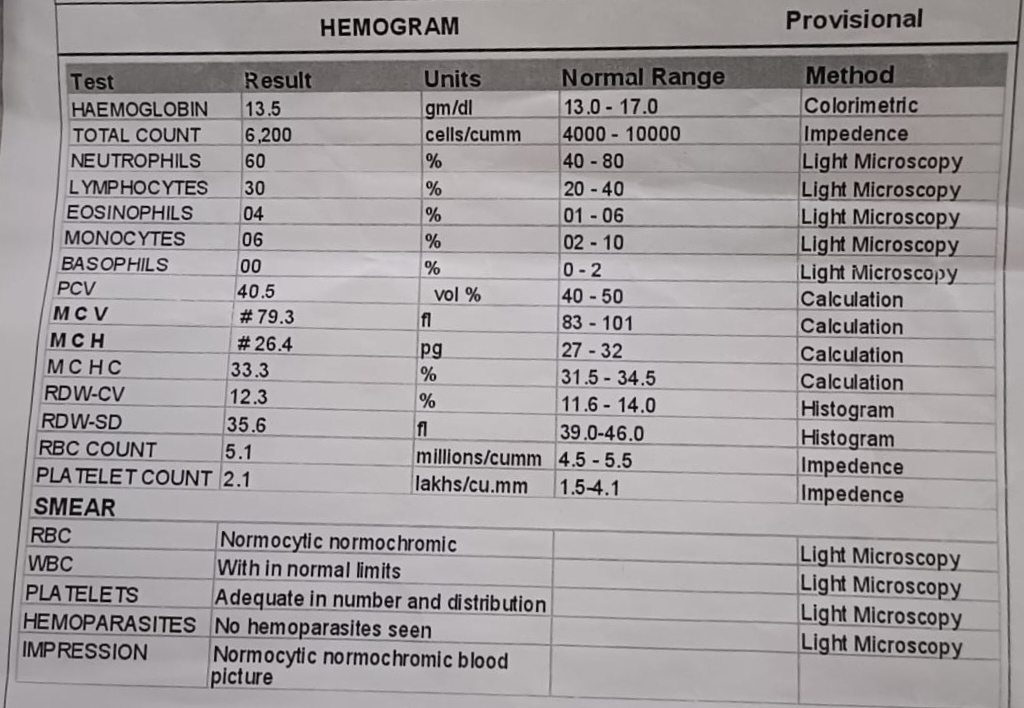
Complete blood picture
Liver function test
Renal function test
Blood grouping
ECG
Chest x ray
Random blood sugar
Complete urine examination
HIV
HBsAg
dropping of right shoulder :
Provisional diagnosis :
right side pleural effusion with lung collapse.
Tubercular pleuritis
Treatment :
IV FLUIDS NS 50ML/HR with 1 AMP OPTINEURON
INJ.NEOMOL 1GM IV /SOS IF TEMP >101 F
T.PCM 650 MG PO SOS
INJ.TRAMADOL 1 AMP IN 100ML NS SOS
T.AZITHROMYCIN 500MG PO/OD
INJ PAN 40 MG IV/OD
TAB.ATT 4tab po/of
H 5mg/kg 340mg
R 10mg/kg 680mg
Z 25mg/kg 1700 mg
E 15mg/kg 1020mg

Comments
Post a Comment